
Nutrition & Supplements
The Philosophy
Every bite during pregnancy is building a human being. Prioritize nutrients per bite, not calories or volume. Your baby will take what it needs from you first — if your diet doesn't supply it, your own reserves pay the cost. That depletion shows up as aches, stretch marks, and postpartum depression.
Anchor your diet around the most nutrient-dense foods: organ meats (especially liver), pasture-raised eggs (2 daily for choline), wild-caught fatty fish (DHA), dark leafy greens, and bone broth. Avoid refined sugar, canola oil, and ultra-processed foods.
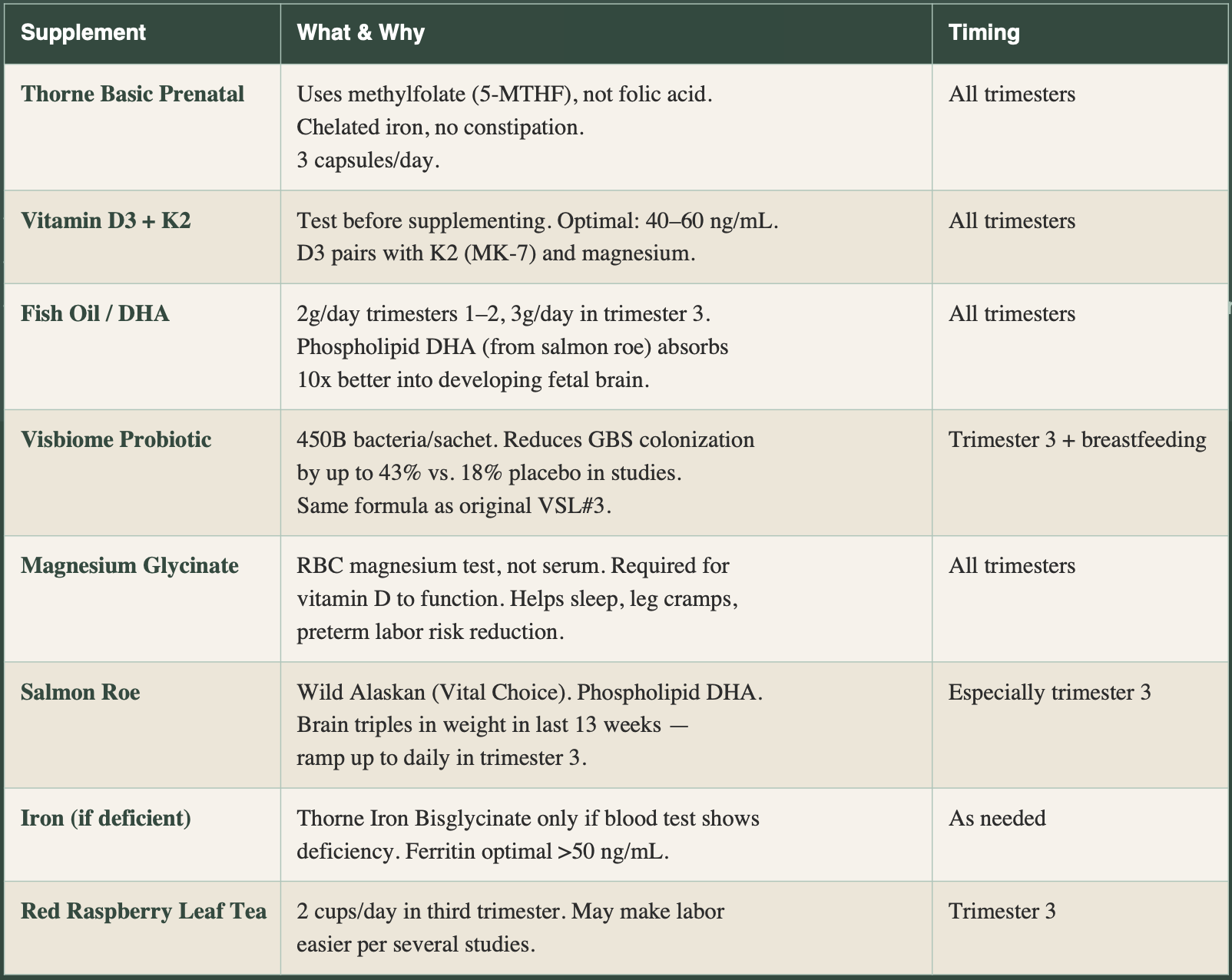
Core Supplements:
Key Blood Tests to Order Yourself
Most insurance will not cover these as they fall under “revention”, but they are well documented as important for birth and pregnancy. Even out of pocket is not that crazy of a cost. Consider $100 now to prevent thousands of dollars and heartache if a problem does occur.
Order online through labs like:
Ulta Lab Tests (ultalabtests.com) or
Marek Diagnostics without a prescription. ~$100–300 total.
The things to be studied:
Ferritin (iron storage) Optimal >50 ng/mL preconception, ideally 80+. Standard labs only flag <15.
25-Hydroxy Vitamin D Optimal 40–60 ng/mL. Conventional 'normal' (20 ng/mL) is too low for pregnancy.
Full thyroid panel TSH, free T4, free T3, TPO antibodies. TSH optimal 0.5–2.5 mIU/L in pregnancy.
Homocysteine Optimal 3.9–7.3 mmol/L. Elevated = methylation problem. Fix with methylfolate + B12.
MTHFR genetic test 40–49% carry one copy; 13–24% carry two. Two copies = can convert as little as 30% of folic acid.
Magnesium RBC Not serum. Deficiency linked to preterm labor, preeclampsia, poor sleep.
What to Read & Watch
Books
Real Food for Pregnancy — Lily Nichols. The best prenatal nutrition book available. Evidence-based, ancestral-informed. Also on Audible.
Ina May's Guide to Childbirth — Ina May Gaskin. Hundreds of natural birth stories. The antidote to fear. Read this first.
Babies Are Not Pizza — Rebecca Dekker. Evidence-based breakdown of hospital birth norms. PhD clinician turned birth advocate.
Natural Hospital Birth - How to prepare for a natural birth in a hospital setting
The Birth Partner — Penny Simkin. The partner manual. Every dad should read this.
Expecting Better — Emily Oster. Economist analyzes the pregnancy research. Great for the data-minded. But I did have a few objections to her conclusions, which tend to favor the data which is incomplete, often overlooking more natural generational midwifery knowledge that has not bee studied officially. But in general, a lot of interesting data (I just happen to come up with different conclusions with that same data).
Womanly Art of Breastfeeding — La Leche League. The breastfeeding reference. Comprehensive and practical, but also a surprisingly fun read.
Transformed by Birth — Britta Bushnell. For the mental and emotional preparation. Approaches birth as initiation.
Documentaries
The Business of Being Born — Ricki Lake. Amazon Video. The essential film on the US maternity system.
More Business of Being Born — Four-part follow-up series. Amazon Video.
The Devil We Know — On PFAS/Teflon. Relevant to cookware and toxin reduction in pregnancy.
Birth Classes (In addition to Hospital Provided Classes)
Hospital birth classes teach you to be a good patient. They do not teach you the physiology of undisturbed labor, your
rights, or the evidence behind common interventions. Take a third-party class instead.
Evidence Based Birth — evidencebasedbirth.com — PhD-led, 300+ podcast episodes, printed guides. For the research-minded.
Mama Natural — mamanatural.com — Week-by-week program, videos, zoom calls. Warm and accessible.
Birthing from Within — birthingfromwithin.com — More holistic/emotional preparation.
Spinning Babies Class — spinningbabies.com/online-classes — $27 online. The single best hour you can spend understanding how babies move through the birth canal. Required viewing.
Podcasts & Online Resources
Evidence Based Birth Podcast — 300+ evidence-based episodes on every birth topic imaginable.
Spinning Babies Daily Essentials — spinningbabies.com — Free daily exercises for optimal fetal positioning.
The Miles Circuit — milescircuit.com — Specific sequence for encouraging baby into optimal position.
FoundMyFitness (Rhonda Patrick) — foundmyfitness.com — Deep dives on DHA/phospholipid, probiotics, vitamin D in pregnancy.
Preparing Your Body
Posture & Alignment
The goal is to keep the heaviest part of the baby — their spine and back — facing your belly button. Think of your belly button as a flashlight that should always point toward the floor. Spine-on-spine (baby sunny side up) is what causes back labor and stalls.
Avoid reclining on soft couches — sit upright or on a birth ball instead.
Avoid long car rides, especially in the third trimester.
Cross your legs forward, not backward. Keep pelvis open.
Sleep on your left side with a pillow between your knees.
At your desk, keep hips higher than knees. Sit forward.
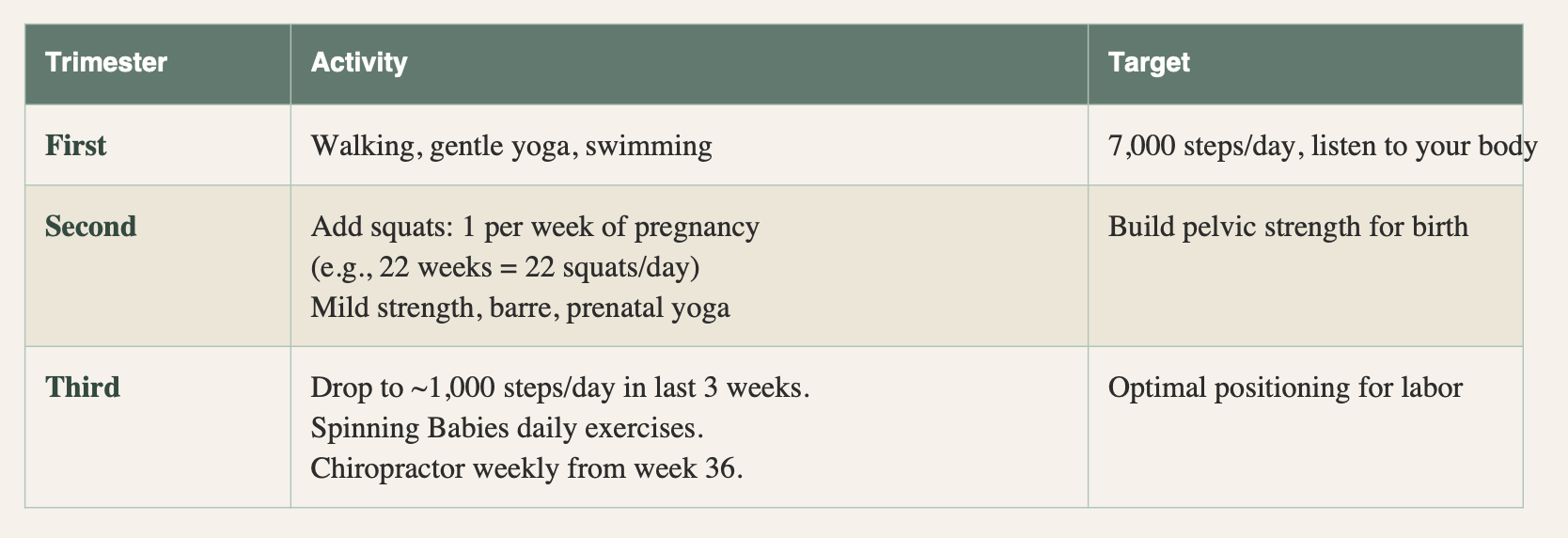
Movement & Exercise
Specialist Support
Chiropractor (Webster certified)
My #1 recommendation for someone to see in person.
Find someone who specializes in pregnancy. Every other week from week 22, weekly from week 30. Aligns pelvis so the baby has the easiest path out. Worth every penny. Look for a woman practitioner who does Webster technique, and who is familiar with the Spinning Babies program.
Bonus if they are called a “chranial sacral” therapist
Pelvic Floor Physical Therapist
Before AND after birth. Gets a baseline of your pelvic floor, identifies any specific areas to work. This is standard in care in France (visited in the home 4 days, 8, days, and 15 days after birth, not just the 6 week checkup in America)
Covered by most non-Kaiser insurance. Prevents postpartum issues with running, incontinence, and recovery.
Acupuncturist
Optional but helpful for stress, sleep, and going past 40 weeks naturally. If you're past 41 weeks, acupuncture can encourage labor to start without synthetic hormones.
I only attended once, when I was having trouble sleeping, and it did indeed help me relax. I asked her how it worked, and she said nothing is direct as in, come in for sleep, it is more about getting your blood to flow and help with relaxation, and when your nerves relax and stress hormones reduce in your bloodstream, many downstream complaints subside.
On dates: Eat 6 Medjool dates per day starting at 36 weeks.
Studies show dates significantly reduce the need for induction and shorten early labor. Only if GBS negative.
Nipple Stimulation (and more)
Begin nipple stimulation with a breast pump at 40+ weeks to naturally encourage labor. (Sexual acts are actually encouraged even when labor begins. Sex in itself is a natural relaxer. You cannot have an orgasm if you are stressed. There is a link with relaxation and allowing your body to accept love and good things).
Interventions Explained
You will be offered — or simply handed — a series of standard interventions from the moment you arrive at triage. Knowing what each one is, why it is offered, and what the evidence says means you can make real decisions rather than defaulting to whatever reduces friction. If you don't know your options, you don't have any.
Monitoring
Continuous Electronic Fetal Monitoring (CEFM): Standard hospital default. Keeps you tethered, limits movement. Research supports intermittent monitoring as equally safe for low-risk births. Ask for intermittent per ACOG guidelines.
Telemetry / Wireless Monitoring: If continuous monitoring is required, ask for wireless telemetry — allows movement, which is critical for labor progress.
Fetal Scalp Electrode (FSE): A small electrode screwed into baby's scalp for continuous internal monitoring. Only appropriate if external monitoring cannot get a clear read for 5+ minutes. Not a routine intervention.
IUPC (Intrauterine Pressure Catheter): Measures contraction intensity internally. Only relevant if labor stalls and provider wants to confirm contractions are strong enough to dilate cervix (target: 200 Montevideo units). Decline unless clinically indicated.
Cervical Exams
Each internal exam after your water has broken introduces bacteria and increases infection risk. You are entitled to decline exams. Typical acceptable windows: one at triage to assess dilation, one before pushing begins. The number is negotiable — you set the terms.
Remember, YOU hire the doctor and hospital. You are not required to do ANYTHING. They are there to support you.
Induction Cascade
Inductions are needed to help get you to 3 cm dilated. If you get there on your own, you don’t need any of these. This is why laboring for as long as possible at home is great, since you are most comfortable in a familiar setting and can walk around, etc. The first pregnancy takes a little longer, so less chance of an uber birth (more common in subsequent births).
If induction becomes necessary, it typically follows this sequence. Understanding it helps you know where you are and what each step means.
Cervical Ripening Agent: Cervidil (FDA-approved, vaginal insert, dosed every 2 hours for 12 hours) or Misoprostol/Cytotec (NOT FDA-approved for pregnancy but used widely — serious side effect risk including uterine rupture). Ask specifically which one and why. Foley bulb (mechanical dilation to 3–4cm) is another option.
Pitocin (synthetic oxytocin): Starts labor or augments stalled labor. Unlike natural oxytocin, Pitocin does NOT trigger the endorphin response. Contractions become more intense without the natural pain relief that should accompany them. This is why Pitocin reliably leads to epidural requests. Some women need only 1 unit; others require 20. You can ask to start low and increase slowly.
Many of my friends were progressing along beautifully in labor and contractions, then when they got to the hospital, were routinely given Pitocin to “speed things along”. This causes unnaturally intense contractions, seemingly out of the blue for the mom, which makes her more likely to ask for an epidural. It caused my friend to have an unwanted C-section and a really tough recovery (another mom had an infection and was bedridden and felt awful for 3 weeks). Another had a spinal tap intense migraine for months from epidural gone wrong. Know every intervention has possible side effects. The key note here, is if you are progressing fine, and even if labor stalls a little from the moving in the car and into the sterile bright lights of a hospital, try to get back into your head first, before accepting pitocin. Protect that IV in your arm, even reject it like I did, so that if they have to put something in you, they have to ask first.
PROM (Premature Rupture of Membranes): If your water breaks before contractions begin: 75% of women go into labor within 24 hours without intervention. You can ask your provider if there is wiggle room to labor at home before coming in. Hospital will typically push for immediate induction — ask about timing and evidence.
Note: 41 weeks and 3 days: This is the physiological average due date — 50% of women go past 41 weeks. Hospitals often pressure induction before this. GBS positive women should discuss timing carefully. GBS negative: dates + acupuncture + nipple stimulation first.
On the IV line: Hospitals prefer a prophylactic IV (saline lock) for liability. You can decline or negotiate. If you agree to a partial bag, know that IV fluids cause swelling in mother AND baby. This inflates birth weight — and the subsequent apparent 'weight loss' in days 2–3 is often just fluid loss, not a breastfeeding failure. Ask them to put it on the outer wrist and confirm what will and won't be added without your explicit consent.
IV tubing plastic contains chemicals not permitted in toys for children under 12 — yet routinely administered to pregnant women. This is worth knowing, and for every person working in a hospital to complain and request for change.
Pain Management Options
Understanding every option before you need to decide removes the biggest source of panic in the labor room. The goal is not to be a hero. The goal is to be informed. The options are always available — knowing them in advance means you choose, rather than react.
There are surprisingly few options. Tylenol does nothing, like a drop of water in an ocean, plus has its own downsides. My best advice is to learn pain management techniques to preserve and protect your body’s natural pain relieving strategies that dissappear once the man made Pitocin (hormone copycat) is added to the equation.
Natural / Unmedicated: Your body produces endorphins in parallel with oxytocin as labor intensifies — a calibrated pain management system. Movement, position changes, water, breath, hip squeezes, and continuous doula support are your tools. Pain ends the moment baby is born. Recovery is typically faster and less complicated.
Best for: motivated, prepared mothers with continuous support. Requires preparation.
Nitrous Oxide (Laughing Gas): Takes the edge off without removing sensation entirely. Does NOT block the endorphin response. Encourages deep breathing which helps in itself. Only the laboring mother can hold the mask — nobody else can hold it for her. Works well in early-to-active labor. Effect wears off quickly.
Best for: wanting some relief without full commitment to epidural. Good bridge option.
Hot Bath: Sometimes included in a birth room. Water helps calm the mom. The basis for water births.
IV Narcotics:
Fentanyl (aka street drugs) lasts ~2 hours. Morphine lasts ~4 hours and is typically offered only early in labor, often to help an exhausted mother rest.
Side effects: changes to baby's heart rate, slowed breathing after birth, lower APGAR scores, reduced breastfeeding behavior in newborn.
Consider: timing carefully — effects on baby at delivery are documented.
Epidural: Regional anesthesia that numbs from waist down. Typically contains fentanyl. Requires continuous monitoring, IV, catheter — you are tethered and cannot move freely. Slows labor by average of 2 hours. Reduces ability to feel and direct pushing. Increases likelihood of further interventions. Ask to turn it down during pushing for more sensation and strength.
Know: ask for the lowest effective dose. You can request it be reduced for pushing.
Understand the side effects, the long list of very common downsides that happen with this, many that go unreported. With a small group of 5 moms, 2 had major negative side effects. You are at the mercy of the skill of the people administering it. I have heard stories of the anasthesia not kicking in or done poorly, the needle going into the wrong place inducing very extremley painful migraines for months after, and many women who are numb in their whole body, not just their legs, making it hard to connect with the baby after.
TENS Unit: Transcutaneous electrical nerve stimulation — adhesive pads on your back delivering mild electrical pulses. Drug-free, can be used at home during early labor. Available to rent or purchase. Particularly useful in early labor before going to hospital.
Best for: early labor at home. Excellent complement to other methods.
The one-more-hour rule:
"Can you get through one more hour?" — This is the mental tool that works in labor when the pressure to accept intervention or pain medication feels urgent. Tell yourself: one more hour. Then reassess. This also works as a polite response to an overzealous doctor: 'Can I have just one more hour before we decide?' Most of the time —yes.
Birth Preferences Checklist
This is not a birth plan — it is a preferences document. Birth is unpredictable. The goal is for your care team to know your values so they can honor them when they can, and discuss trade-offs with you when something changes. Edit as you need it and print. Give a copy to your doula or nurse.
ON ARRIVAL
Partner to answer intake questions so I am not disrupted during contractions
Midwife or OB to perform any cervical exams (decline routine nursing exams)
No students or observers unless I explicitly agree
Music playing when we arrive — keep it going
Minimal questions during active contractions
MONITORING
Intermittent electronic fetal monitoring per ACOG guidelines (not continuous)
Wireless telemetry if continuous monitoring is required
Fetal scalp electrode only if no external heart tone for 5+ minutes
IUPC only if labor has truly stalled and contraction strength is in question
Cervical exams limited — one at triage, one before pushing
IV & FLUIDS
Prefer no prophylactic IV / saline lock
If IV agreed: outer wrist placement, half bag only, nothing added without explicit consent
No routine IV pitocin unless medically necessary
LABOR SUPPORT
Freedom to move, change position, use water, walk
No arbitrary time limits on labor progress
Hip squeeze technique used by partner and doula during contractions
Doula present and included in all discussions
No unsolicited commentary on pain management choices
PUSHING
Coached only if I request it (no cheerleading counts)
Variety of positions — not flat on back
No time limits on pushing as long as baby and I are stable
Perineal warm compress and lubricating oil
Prefer to risk natural tear over episiotomy
Mirror available if I want it
rationalbody.com · Page 11RATIONAL BODY The Rational Birth Guide
IMMEDIATELY AFTER BIRTH
Baby placed skin-to-skin immediately
Delayed cord clamping — wait until cord stops pulsing (5–20 minutes)
Partner to cut cord (unless doula if partner declines)
All routine newborn procedures delayed minimum one hour
First breastfeed before weighing and measuring
No eye ointment until after the first hour
Baby stays in room with us throughout hospital stay
Placenta saved (encapsulation or other)
NEWBORN PROCEDURES
Vitamin K injection: YES (ask for preservative-free version)
Erythromycin eye ointment: delayed / discuss with provider
Hepatitis B vaccine: delay until pediatrician consult
Heel stick metabolic screen: YES (after 24 hours of feeding)
No bath in hospital — bathe at home
Breastfeed exclusively — no formula, bottles, sugar water, or pacifier unless medically necessary
IF CESAREAN BECOMES NECESSARY
Partner present in OR throughout
Gentle cesarean / family-centered cesarean requested
Cord milking or delayed clamping (up to 60 seconds) if possible
Baby skin-to-skin on my chest or partner's during surgery if possible
Vaginal seeding gauze prepared and ready
Breastfeeding within first hour in recovery
All newborn procedures delayed until after bonding
Affirmations for Labor
Print this page. Put it in your go bag, highlight your favorites, post it on the wall of your labor room, in your doula's hands. Short, grounded, easy to repeat. Say them before you need them so they are already in your body when things get hard.
For the Birthing Person
“My body knows how to do this. I just have to get out
of its way.”
“I can't stop the waves, but I can learn to surf.” “Each contraction is bringing my baby closer to
meeting me.”
“These sensations are not stronger than me — they
are part of me.”
“I was born to do this.” “My body is capable and strong.”
“I trust my body. I trust my baby. I trust my birth.”
“My mind is relaxed. My body is relaxed.”
“With each deep breath, I surrender more.”
“My baby trusts me. And their body knows what to
“I am prepared to meet whatever turns my birth
takes.”
“My baby and I are working together.”
do.”
“I am fierce but flexible.” “Each wave has a purpose. Each one is practice.” “I can do anything for one minute.” “People all over the world are birthing with me right
now.”
“Open. Surrender.” “I am safe. My baby is safe. My family is safe.”
“One breath. One surge at a time.”
“I breathe deeply and I am calm.”
“This is the day I've been waiting for. I am ready.”
“I am created to do this.”
For the Partner
“I am a rock for my loved one today.”
“My partner and baby are healthy and strong.”
“My partner is depending on me, and I am ready.”
“My one job today is presence. I am fully here.”
rationalbody.com · Page 13RATIONAL BODY The Rational Birth Guide
“I handle the room. She handles the birth.”
Visualizations:
Riding a wave, surfing on top, soaring, rather than being pummeled by it.
Diving deep into the ocean, below the turbulence, where it is dark and calm. Floating. Taking charge.
Picturing a blossoming flower expand. This helped connect with the images of the birth canal opening.
The pinky door visualization:
Months before my first birth, I slammed my pinky in a door. There is not a whole lot you can do in that instant but just deal with the pain. Instead of recoiling from the pain, I stared at it. I asked: “what is pain, actually? Where is it? What is it doing? The sensation shifted — not gone, but held at a distance, muted. I brought this into the delivery room. During contractions: don't brace against them. Observe them. The contraction is not hurting you. It is working. It is doing exactly what it was designed to do. It is getting your body to push a baby out!!! It needs space, and it is only for a short while then will be over. That baby has to come out somehow!
Newborn Decisions
These decisions happen in the first hours — often when you are holding your baby for the first time and not paying attention to anything else in the room. Decide these before you go in. Put them in your birth preferences. Brief your doula.
Delayed Cord Clamping: The agency WHO (World Health Organization) recommends waiting until the cord stops pulsing — typically 5–20 minutes. One-third of your baby's blood volume is still in the cord at birth, rich in stem cells and iron. People pay tens of thousands to bank cord blood. Your baby deserves it in their body first. A nurse will move to cut automatically — your doula can help pay attention and catch this- help push back on cutting too soon.
Skin-to-Skin (Golden Hour): Baby on your bare chest from the first moment, covered with a warm blanket, for minimum one hour before any routine procedures. This is not preference — it is biology. Temperature regulation, heart rate, cortisol, blood sugar, first feed, milk initiation — all happen here. Healthy newborns can be assessed on your chest without being taken away.
Skin-to-Skin for Father (or partner): As soon as possible after the mother. The oxytocin response is not exclusive to women — a father holding his bare-chested newborn against his bare chest is having a real neurochemical experience that changes how he bonds with and cares for that child. Plus mama needs rest at some point! When mom is sleeping, let someone else hold that baby right on their chest! It is magical. Stare at their eyes, just get lost in the moment. <3
Vitamin K Injection: Newborns are born with low clotting factors. Vitamin K deficiency bleeding — including intracranial bleeding — is rare but serious. The injection is the most effective prevention. Strong evidence for benefit. Ask for preservative-free version. Oral alternative exists but requires multiple doses and is less effective.
Erythromycin Eye Ointment:
I push back on this. It prevents eye infection from gonorrhea or chlamydia passed during delivery. If you tested negative for both during pregnancy, risk is effectively zero. The ointment blurs vision and may interfere with the golden hour visual bonding.
The risk is that some people’s partners may have slept with others since the last time mom was tested. If you don’t think it applies to you, don’t do it. It is becoming standard to push back on this.
Ask to delay until after the first hour, or discuss with your provider whether it applies to you.
Hepatitis B Vaccine: The disease is transmitted through blood or sexual contact. If you tested negative during pregnancy, your newborn's risk is zero. Unless mom is a nurse or prostitute in regular contact with blood, it is most likely not necessary.
Safe to delay to first pediatric appointment. This conversation should happen before delivery, not in the room.
Newborn Metabolic Screen (Heel Stick) Screens for rare but serious metabolic disorders. Do not skip this. Can be done after 24 hours of feeding for best accuracy.
Vaginal Seeding (if C-section): If cesarean becomes necessary, you can request vaginal seeding — swabbing baby with maternal vaginal fluid immediately after birth to approximate microbiome transfer. Prepare gauze in advance. Confirm your provider is willing before delivery day, or find out how to do it yourself.
Breastfeeding: Initiate within the first hour. Colostrum is not a preview of breast milk — it is a completely different substance: dense, golden, packed with immunoglobulins and the exact bacteria to seed the gut microbiome. Supplementing with formula in the first days reduces the milk supply signal. If supplementation is recommended, ask whether it is medically necessary or precautionary, and whether donor breast milk is available.
People pay tens of thousands of dollars for this- it’s no joke. Many babies born as preemies can use it- but it has to be taken from mothers, often those of low income background, at the expense of giving it to their own children, causing a social disparity gap that is not easily filled.
Postpartum & Fourth Trimester:
The hospital stay ends. The books stop here. The hardest part is about to begin — and almost nobody prepares for it. The fourth trimester is the twelve weeks after birth. Your uterus is contracting from the size of a watermelon back to its original size. Your hormones are in the most dramatic flux of your life. You are establishing milk supply on fragmented sleep. You are healing from a marathon while running another one.
The 18-Month Grace Rule: Give each other 18 months of grace after the baby arrives. Whatever is said in this period — say to yourself and to each other: we are both trying. We are both failing by our own standards. We are both doing the most important work in the world. Come back to each other after sleep, after food, after a moment of quiet. Not in the middle of the 3 AM feed.
What You Need in the First Weeks:
Sleep: Sleep deprivation reaches levels comparable to active military personnel. A mother who cannot sleep cannot heal, cannot breastfeed successfully, and is measurably more at risk for postpartum depression. The single best thing anyone can do for you is hold the baby while you sleep for 3+ consecutive hours.
Personally, sleep deprivation caught up to me a year after my second son was born. At that point, he was only waking up once a night or so, but my elder son, around 3 at the time, had consistently been a tough sleeper and always woke up around 5am. The two combined led to me being pretty sick, and I set up an appointment with a naturopath to find out what was going on. I just could not get my engine revving for the day. Turns out the only thing abnormal was my testosterone levels, well below the window of healthy. The practitioner was not surprised, she said this is very common for sleep deprived parents. In fact, body builders can hide the fact they took testosterone by skipping a single night of sleep. That is how sleep dependant this hormone is. Without it, we show all the same symptoms as depression. This made me understand that many forms of depression are rational responses to something our bodies are begging us to get more of, especially sleep.
Warm Nourishing Food: Bone broth. Soups. Protein. Cooked, warm, easy-to-digest food. Traditional postpartum diets worldwide — Chinese zuo yue zi, Indian traditions, Ayurvedic practice — all converge on the same things for the same biochemical reasons.
Set up a meal train before the birth. Accept every offer. Freezer baggy meals for the crock pot. Talk to a local religious group to see if anyone can be willing to make some extra meals some nights a week for a low fee. Doordash or hire a chef if you have the resources. Now is not the time to learn to cook if you hate it, see if you can task that out.
3:1 Adult-to-Newborn Ratio: Research from traditional cultures suggests approximately three adults to one newborn is what the early months actually require. A baby genuinely needs that much care. Build this deliberately. A postpartum doula fills part of the gap.
Postpartum Doula: She holds the baby while you sleep. She supports breastfeeding. She makes food. She helps with newborn basics. She watches for warning signs. Daytime: $30–60/hr. Overnight shifts: $200–400. Weekly packages available. FSA/HSA eligible.
Lactation Consultant: If breastfeeding is difficult — and it may be — a private IBCLC lactation consultant is worth the cost. Hospital lactation consultants have 20 minutes and 10 patients, and can sometimes take months to book. The first 5 days are critical. A private consultant has as long as you need. We paid $350 for someone to meet us in our home and feel like she saved us in that moment when our son would not latch. She wrote out notes for me on how to use my breast pump. She helped establish a sleeping arrangement with my husband so I could get at least one segment of 3-4 hours of sleep in a day.
Pelvic Floor PT: Begin at 6 weeks postpartum. Earlier if cleared. Covered by most non-Kaiser insurance. Essential for recovery, return to exercise, and preventing long-term issues.
In Europe, this is standard of care. In home visits at 3 days, 7 days, 15 days, and more. Not waiting 6 weeks. Right away.
Postpartum Nutrition Priorities
Iron Dramatically redirected to baby during pregnancy. Replenish with grass-fed liver, red meat, dark leafy greens.
Vitamin D3 Continue supplementing. Breast milk alone is insufficient for baby — add Carlson Baby D3 drops (400
IU/day) for nursing infants.
DHA / Fish Oil Increase to 3g/day while breastfeeding. Critical for baby's continuing brain development.
Iodine Baby receives it through breast milk — it must come from your diet. Seaweed, fish, dairy.
Choline Baby's brain development. Two eggs daily. Liver. Continue prenatal with choline.
Zinc Wound healing and immune function. Meat, shellfish, pumpkin seeds.
Continue Visbiome 1 sachet/day through breastfeeding. Reduces inflammatory biomarkers in breast milk and improves colic outcomes.
Skin After Birth
Your skin barrier has been under enormous physiological stress. The same biomimetic philosophy that applies to newborn skin applies to yours. Tallow-based balms — grass-fed rendered tallow as in Rational Body's formulations — match the fatty acid profile of your own sebum and deliver fat-soluble vitamins A, D, E, and K directly into tissue that needs all of them.
For nipples: Apply after feeding, not before. Grass-fed tallow, medical-grade lanolin, or calendula-infused apricot oil. Nothing with synthetic fragrance or essential oils near your newborn's face. Baby finds the breast by smell — do not interfere with that navigation before a feed.
For newborn skin: No alkaline soaps (including castile soap and most baby soap). Newborn skin pH is 6.0 at birth, dropping to 5.1 by 6 weeks. Alkaline cleansers disrupt this. Use pH-matched cleanser (5.3–5.7) or plain water. No synthetic fragrance. No essential oils.
You are the expert on your own body.
The doctors know emergencies. The research knows birth. You know yourself.
I wasn't special. I was prepared. That preparation is available to anyone who wants it.
This guide is part of the “Hard Now, Easy Later” birth series by Victoria Siegel · Rational Body · rationalbody.com