Birth, Data, and the System We Built
Are We Actually Better Off? What the Numbers Say — and Why It Matters
By Victoria Siegel | Community Herbalist & Founder of Rational Body
A note before we begin: This is a fairly heavy topic. Nobody wants to think about worst-case scenarios. But I wanted to understand the worst in order to find the best practices.
Yes, we are safer than we were 100 years ago. The reasons for that are specific and worth understanding — detailed below. But compared to other developed countries today, we have some of the worst birth outcomes in the wealthy world, and we spend the most money on it. And when you run the arithmetic on what "matching the best" would actually mean, the numbers are staggering:
If the United States matched the birth outcomes of the best-performing wealthy nations, we could save approximately 14,000 babies and roughly 600 mothers EVERY SINGLE YEAR.
That is not a rounding error. That is 14,000 children who would have their first birthday. That is 600 families who would still have their mother. Every year.
And beyond the numbers: the experience of birth matters. We can shift what is for many women a frightening, disempowering experience — navigating the unknown, in a clinical environment, with little preparation — into one of the most extraordinary moments of a woman's life. With some mental and physical preparation, that shift is genuinely possible. That, too, is worth fighting for.
Where We Are: The Honest Baseline
Birth in America is extraordinarily safe. Let's start there, because that is the true baseline, and anything else would be dishonest.
But any death is a tragedy.
And we have gotten better. A mother walking into a U.S. hospital today faces a risk of dying that is more than forty times lower than it was a hundred years ago. Infant survival has improved by more than 98 percent in the same period. These are genuine, remarkable achievements of public health, medicine, and science.
But when there is a large population — 3.6 million births per year — even a small rate gap translates into a very large number of real people. A fraction of a percent sounds negligible. Multiplied by millions, it is thousands of lives.
And when you compare the United States to the best-performing wealthy nations today — countries with the same technology, the same access to surgical care, the same medical education — the numbers reveal a gap that should not exist.
I started this research genuinely uncertain. As an engineer, I wanted the data, and I wanted to follow it wherever it led — even somewhere inconvenient. What I found is that the story is considerably more complicated than either side of the natural birth debate usually acknowledges.
We are dramatically safer than we were in 1900. But we are not optimized for low-risk birth. The system excels at rescue. It struggles with getting us to 100%.
What I Wanted First and Foremost
I want to be clear about my own priorities before diving into the data, because I think this often gets lost in the natural birth conversation.
I wanted a hospital birth. I wanted it as natural as possible. But first and foremost — before any of that — I wanted a healthy baby.
Many people say it doesn't matter how the baby gets here, as long as the baby arrives safely. I understand that instinct. But the experience matters, too. It matters for recovery. It matters for bonding. It matters for breastfeeding. It matters for the mother's sense of herself as she steps into one of the most demanding roles of her life. And as the data shows, how we give birth has measurable consequences for outcomes — for mother and baby both.
Evidently, this is something more people need to be talking about.
The Big Win: What Modern Medicine Actually Accomplished
First, let's be precise about what drove the dramatic decline in maternal and infant mortality over the 1900’s. Nuance matters here — the story is often told in ways that credit the wrong things.
Antibiotics — particularly sulfonamides introduced in the late 1930s — drove a steep drop in puerperal sepsis, historically one of the leading causes of maternal death. Blood transfusion and improved hemorrhage management addressed another major killer. Improved sanitation in hospitals, and eventually clean water and milk supply in communities, reduced infant and maternal infections dramatically. Better neonatal support — temperature control, respiratory assistance, sterile technique — reduced early infant deaths.
The key point is this: the mortality revolution was driven primarily by infection control, emergency rescue capability, and public health infrastructure — not by treating every labor as a pending emergency from the start.
A historical footnote that doesn't get nearly enough attention: Ignaz Semmelweis demonstrated in the 1840s that handwashing by physicians reduced maternal deaths dramatically — and was largely ignored, even ridiculed by the medical establishment, for decades. The women dying from puerperal fever in hospital settings were in many cases dying at higher rates than women delivering at home with midwives, because hospitals concentrated infection. Germ theory eventually changed that. But the lesson embedded in that story — that an institution's default practices are not always the safest option, and that the people most invested in the status quo are often the last to accept evidence against it — is one worth carrying into the modern conversation.
That distinction matters enormously when evaluating what modern birth practices should look like for low-risk women. We know what saved lives. It wasn't the epidural.
The 50% Figure — and What It Actually Means
At some points in history, infant mortality approached 50%. That number is so staggering that it's easy to read it as evidence that birth itself was catastrophically dangerous — that what saved us was the modern hospital, the obstetrician, the surgical suite.
But when you look at when those babies were dying, the story changes.
A significant portion of historical infant deaths did not happen during birth. They happened in the weeks and months afterward — from infections, contaminated water, and a food source that was never meant for human infants, handled in conditions that made it deadly.
That food source was cow's milk.
In the late nineteenth and early twentieth centuries, as urbanization separated families from farms and wet nursing became less common, cow's milk became the default infant food. This milk was often unpasteurized, unrefrigerated, transported in conditions that allowed dangerous bacterial growth, and fed to newborns whose immune systems were completely unprepared for it. The summer infant mortality spike that early public health workers documented was substantially driven by bacteria thriving in unrefrigerated milk transported by wagon in summer heat. Contaminated cow's milk killed enormous numbers of babies — not in the delivery room, but in the weeks that followed. Pasteurization, refrigeration, and improved sanitation of the milk supply dramatically reduced those deaths.
What does pasteurized cow's milk have to do with whether natural birth is safer than medicated birth? Nothing. Absolutely nothing. But those infant deaths are folded into the same historical statistics that get cited to argue for the superiority of modern obstetric intervention over traditional birth. The categories collapse in ways that obscure what actually happened.
Mother's milk, fresh from the breast, carried none of those risks. It requires no refrigeration, no supply chain, no clean water to mix, no careful handling between source and infant. Breastfed babies were not dying from contaminated food in those summer months. The babies dying were predominantly formula-fed.
Breastfeeding rates declined sharply through the early and mid-twentieth century — partly because of formula marketing, and partly because the medicalization of birth itself undermined it. Women who had been anesthetized during delivery were in no condition to nurse immediately afterward. Babies taken to nurseries rather than placed skin-to-skin missed the biological window that establishes early latch. Hospital routines prioritized staff convenience over the timing the nursing relationship requires. When breastfeeding rates fell and cow's milk filled the gap, outcomes for some babies got worse, not better.
So when we say modern medicine saved babies — yes, in many important ways it did. Sanitation saved babies. Clean water saved babies. Pasteurization made a dangerous substitute marginally safer. Antibiotics saved babies. Better maternal nutrition saved babies. But the specific interventions in the birth room are only one part of that story, and not always the most important one. Separating those threads matters if we want to understand what is actually helping — and what is getting credit it doesn't entirely deserve.
Then vs Now vs Best: The Numbers in Plain Units
Below is a straightforward comparison — normalized to the same unit so all three eras can be read side by side.
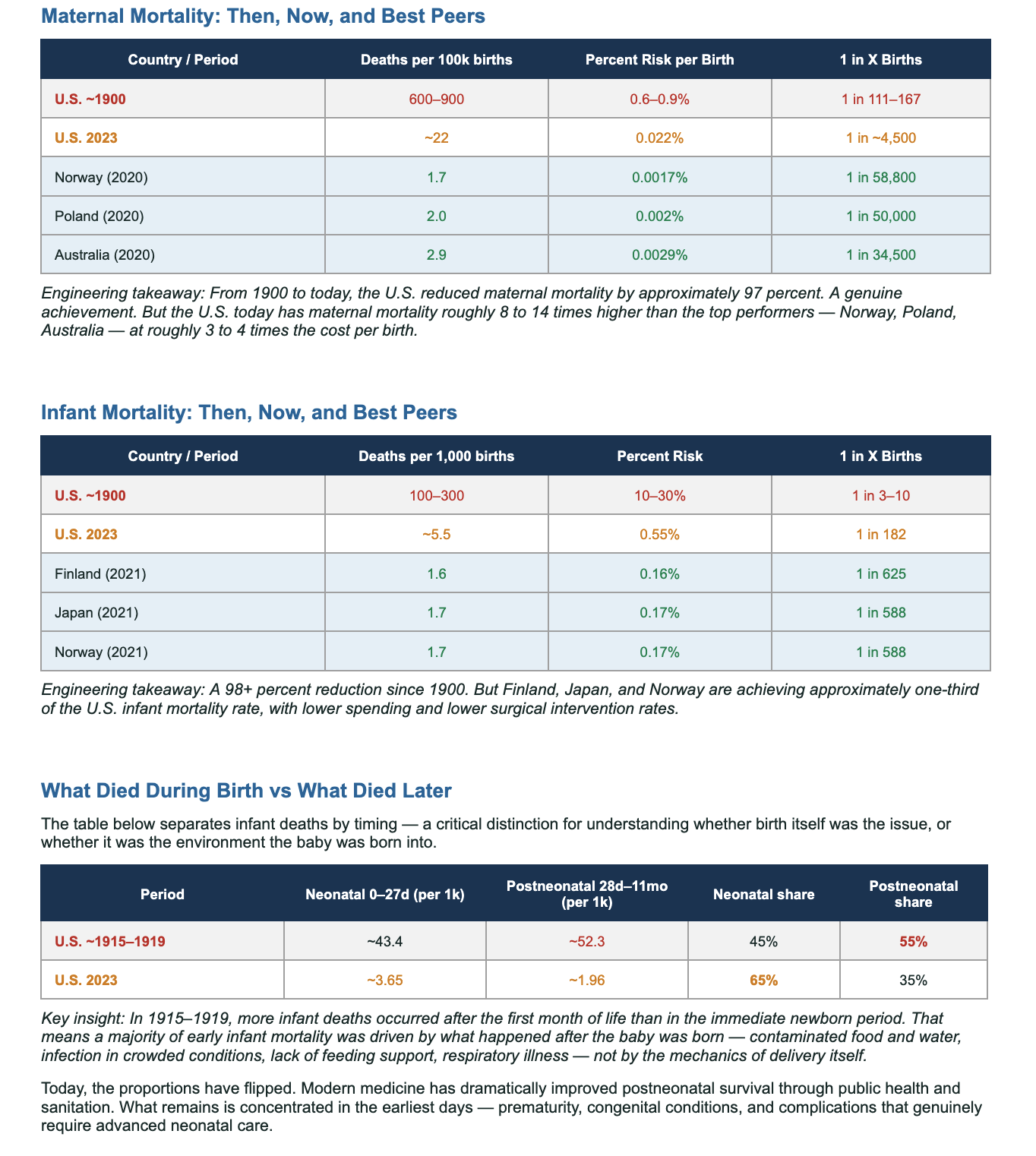
Maternal Mortality: Then, Now, and Best Peers
(Deaths per 100,000 live births)
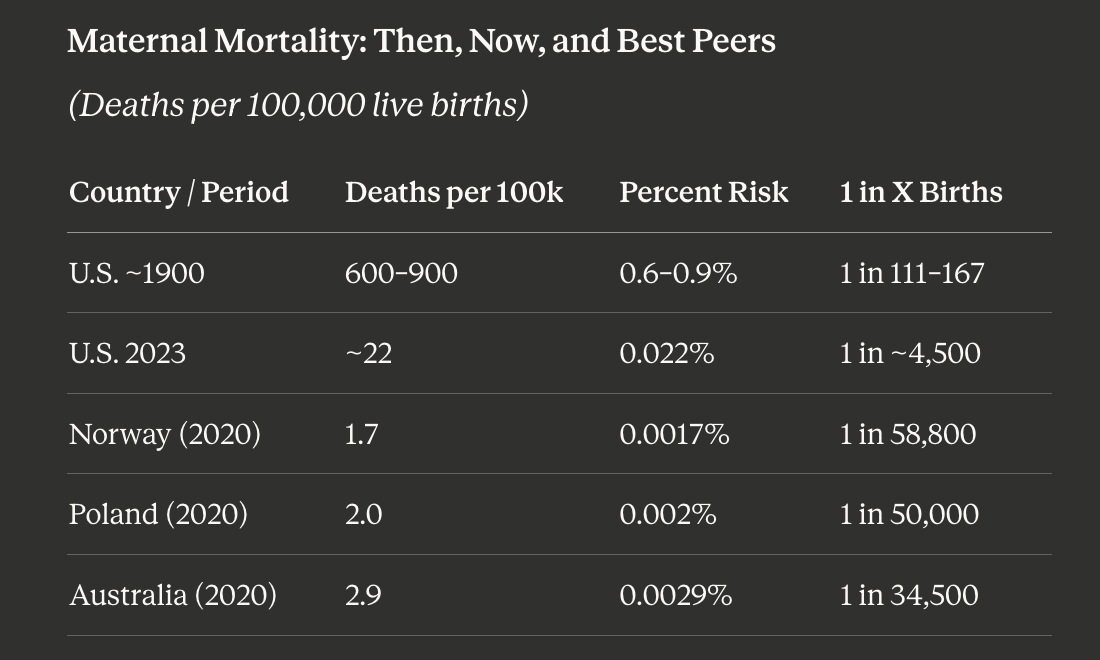
Engineering takeaway: From 1900 to today, the U.S. reduced maternal mortality by approximately 97 percent — a genuine achievement. But the U.S. today has maternal mortality roughly 8 to 14 times higher than the best-performing peer nations, at roughly 3 to 4 times the cost per birth.
Infant Mortality: Then, Now, and Best Peers
(Deaths per 1,000 live births)

Engineering takeaway: A 98+ percent reduction since 1900 — remarkable. But Finland, Japan, and Norway achieve approximately one-third the U.S. infant mortality rate, with lower spending and lower surgical intervention rates.
Who Died During Birth vs Who Died Later
This table separates infant deaths by timing — a critical distinction for understanding whether birth itself was the issue, or the environment the baby was born into.
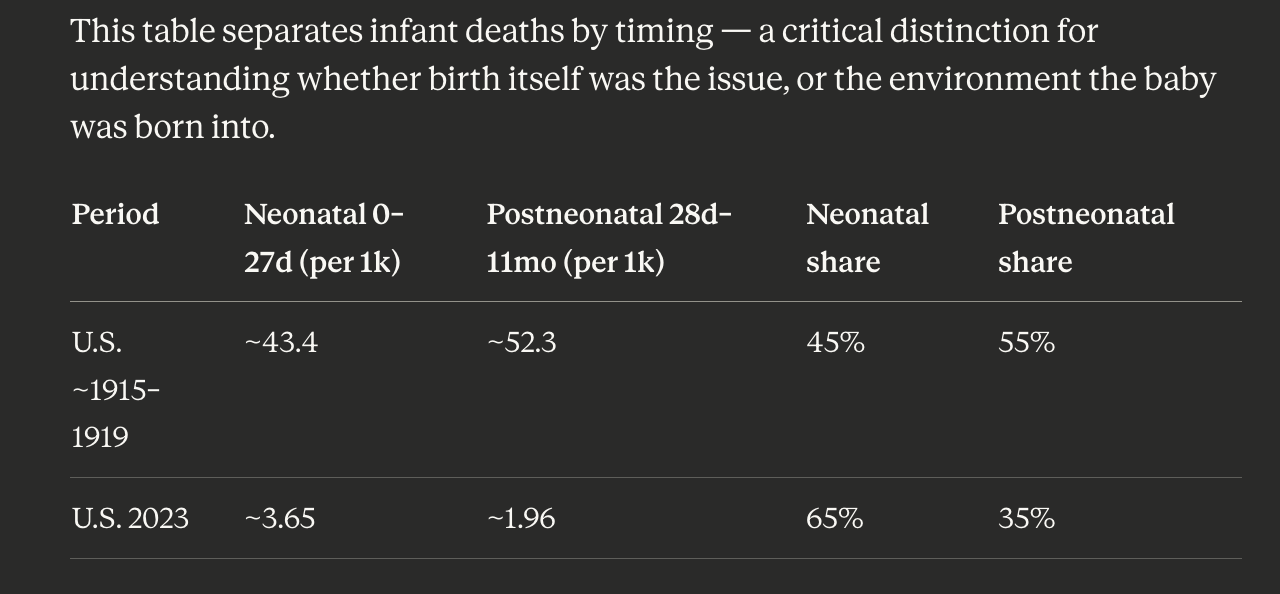
Key insight: In 1915–1919, more infant deaths occurred after the first month of life than in the immediate newborn period. A majority of early infant mortality was driven by what happened after the baby was born — contaminated food and water, infection, lack of feeding support — not by the mechanics of delivery itself.
Today, the proportions have flipped. Modern medicine has dramatically improved postneonatal survival through public health and sanitation. What remains is concentrated in the earliest days — prematurity, congenital conditions, and complications requiring advanced neonatal care.
It is not accurate to credit obstetric intervention for the full historical decline in infant mortality. Much of what we gained, we gained outside the delivery room.
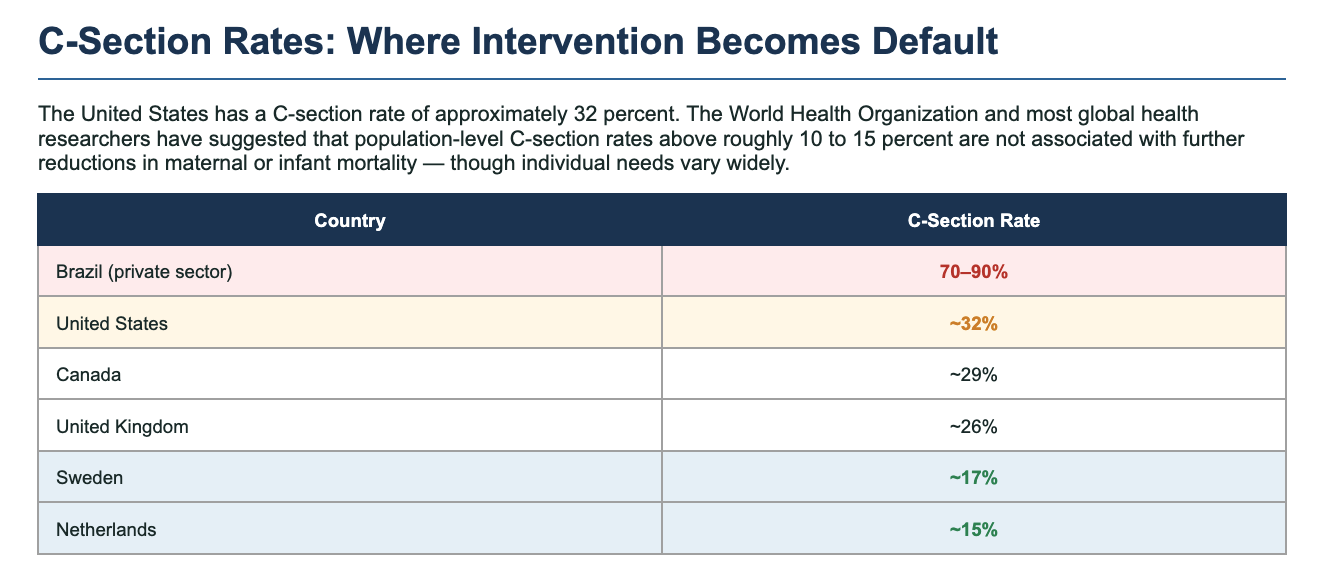
C-Section Rates: Where Intervention Becomes Default
The United States has a C-section rate of approximately 32 percent. The World Health Organization and most global health researchers have suggested that population-level C-section rates above roughly 10 to 15 percent are not associated with further reductions in maternal or infant mortality.
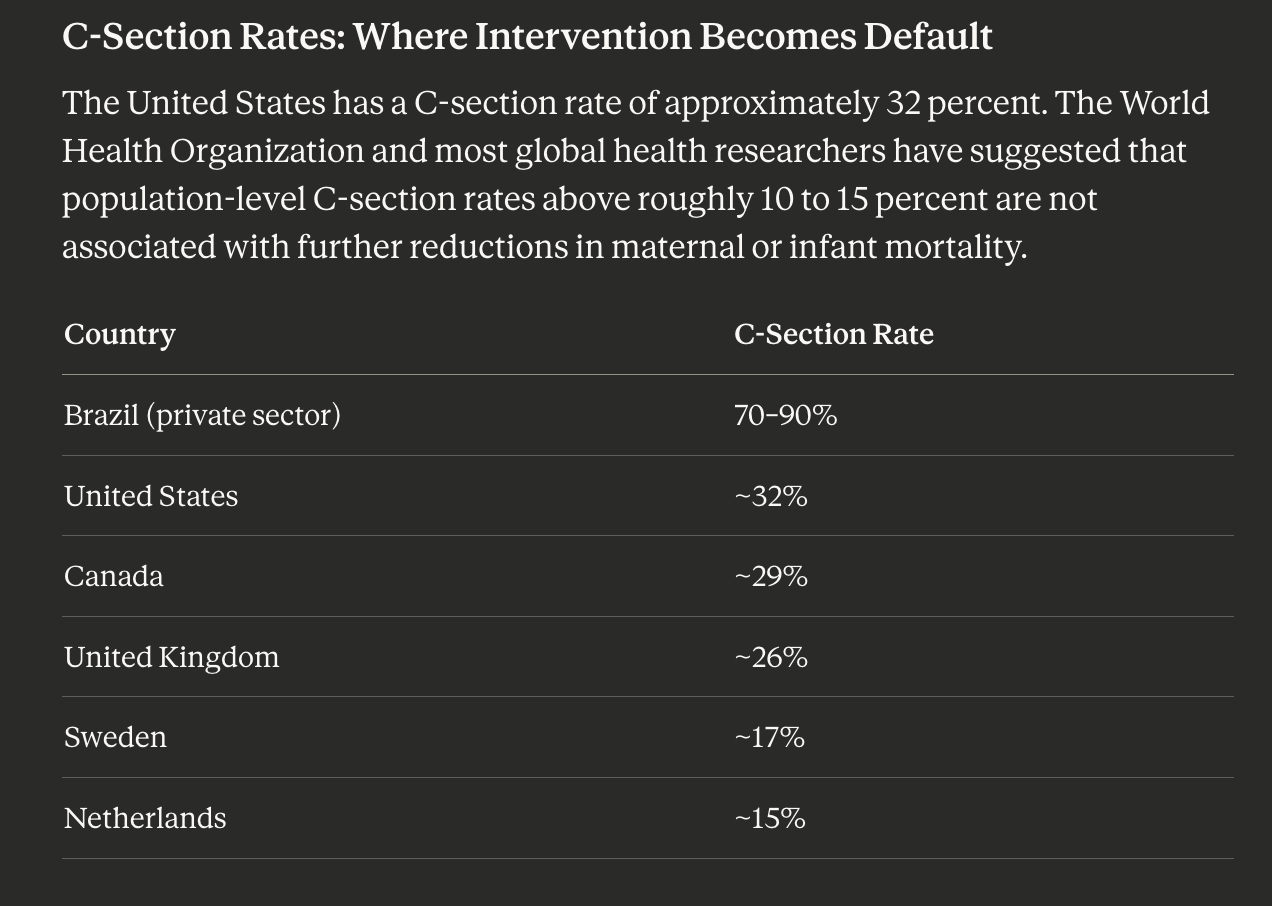
Brazil's private-sector hospitals — where C-section rates have reached 70 to 90 percent — serve as an international case study in what happens when surgical delivery becomes culturally normalized. Outcomes are not better. They are measurably worse. The rate has come entirely untethered from clinical indication.
The United States is not Brazil. But the trend line is worth examining.
There is a financial reality almost never discussed openly: C-sections generate higher reimbursement for hospitals than vaginal births in most U.S. payment structures. At the same time, hospital C-section rates are tracked as a quality metric — because persistently high rates signal over-intervention. The incentives and the outcomes data do not always point in the same direction. A woman who understands both is better equipped to navigate what she is told in the labor room.
And the costs of cesarean delivery go beyond recovery time. Babies born by cesarean miss exposure to the vaginal microbiome that seeds their gut bacteria — a foundational component of lifelong immune development. Mothers recovering from cesareans face six or more weeks of major abdominal surgical recovery at the exact moment when bonding, breastfeeding, and the exhausting work of newborn care demand everything they have. These are real costs. They belong in the conversation every time a cesarean is discussed as a convenience or a preference rather than a medical necessity.
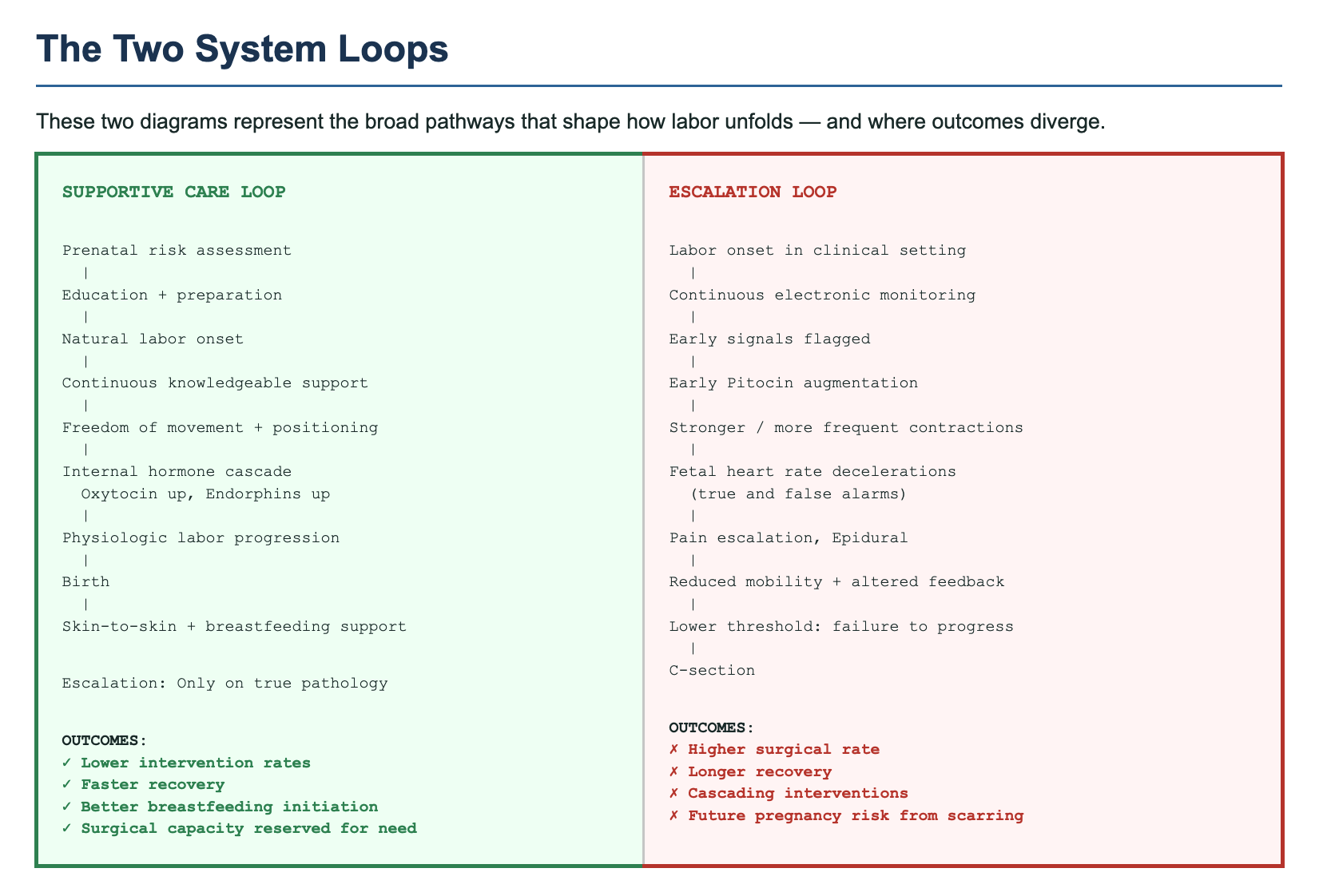
The Two System Loops
These two pathways represent how labor tends to unfold — and where outcomes diverge.
The Supportive Care Loop
Prenatal risk assessment → Education and preparation → Natural labor onset → Continuous knowledgeable support → Freedom of movement and positioning → Internal hormone cascade (oxytocin rising, endorphins rising with it) → Physiologic labor progression → Birth → Skin-to-skin and breastfeeding support. Escalation occurs only on true pathology.
Outcomes: Lower intervention rates. Faster recovery. Better breastfeeding initiation. Surgical capacity reserved for genuine need.
The Escalation Loop
Labor onset in clinical setting → Continuous electronic monitoring → Early signals flagged → Early Pitocin augmentation → Stronger, more frequent contractions → Fetal heart rate changes (true and false alarms) → Pain escalation, epidural → Reduced mobility and altered feedback → Lower threshold for "failure to progress" → C-section.
Outcomes: Higher surgical rate. Longer recovery. Cascading interventions. Future pregnancy risk from uterine scarring.
Neither loop is inherently wrong. Emergency escalation is essential and lifesaving. The question is whether the Escalation Loop has become the default — applied routinely to physiologic birth rather than reserved for true deviation.
The mechanism matters here. Natural oxytocin acts in both the bloodstream and the brain — triggering contractions, yes, but also triggering endorphins, the body's own pain management system calibrated precisely to the intensity of each contraction. Pitocin, the synthetic version, only acts in the bloodstream. It makes contractions happen harder and faster than the body would naturally produce, while the endorphin pathway stays closed. The body reads the synthetic flood as sufficient oxytocin and stops producing its own. The pain intensifies. The natural relief doesn't come. The epidural follows. Mobility ends. The threshold for "failure to progress" drops. Each step makes the next more likely.
This is not theoretical. It is a clinical pattern that researchers have documented and that ACOG has guidelines specifically addressing.
"One system prioritizes physiology first, with escalation for real pathology. The other treats every birth like a pending emergency until proven otherwise. That difference explains why interventions cluster, even when biology didn't fundamentally change."
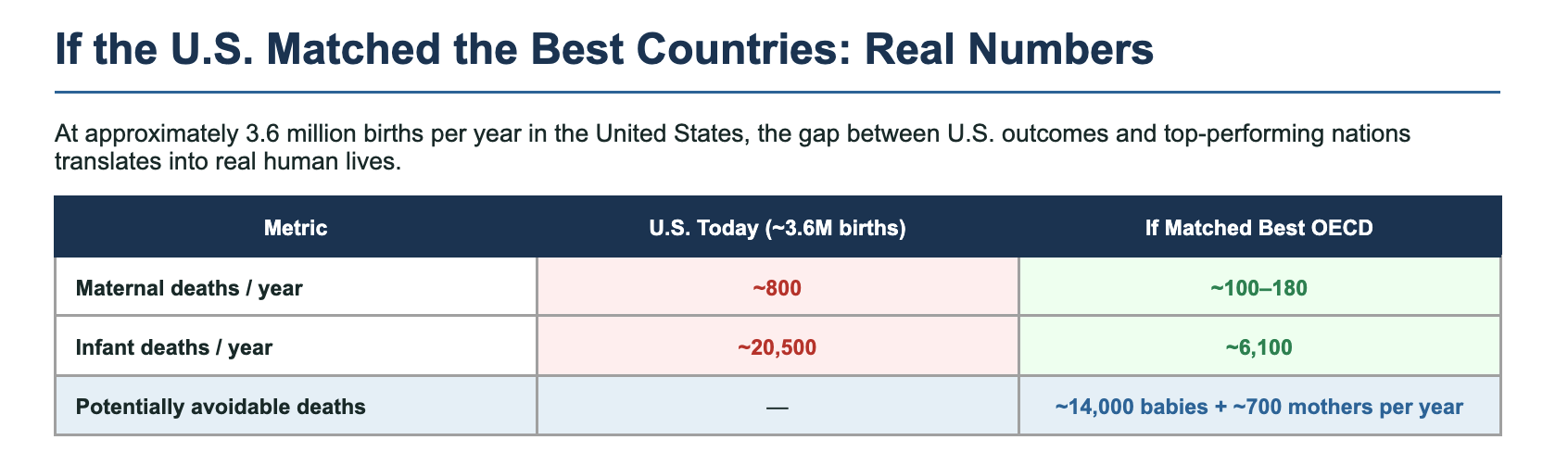
If the U.S. Matched the Best Countries: Real Numbers
At approximately 3.6 million births per year in the United States, the gap between U.S. outcomes and top-performing nations translates into real human lives.

Potentially avoidable — ~14,000 babies + ~700 mothers per year
This is arithmetic, not advocacy. If the United States achieved the same maternal and infant mortality rates as Norway or Finland, approximately 14,000 more babies and 700 more mothers would survive each year.
Not because Norway and Finland are anti-medicine. They have hospitals, obstetricians, and emergency capability. The difference is in how they organize care for the majority of low-risk births — and how much they invest in midwife-led continuity of care, postpartum follow-up, breastfeeding support, and social infrastructure around the new family.
They spend two to three times less per birth. They save two to three times more lives. The perception that more spending and more intervention equals more safety is not supported by the data.
What the Best Countries Do Differently
Midwife-led care for low-risk pregnancies, with clear pathways to obstetric escalation when needed — rather than OB-managed care as the default for everyone.
Continuity of care: the same small team across prenatal visits, labor, and postpartum — reducing the protocol-driven escalation that comes from providers who don't know the patient and are managing liability rather than a person.
Universal coverage with strong postpartum follow-up — catching hemorrhage, hypertensive complications, and infection before they become emergencies rather than after.
More conservative thresholds for early labor augmentation.
Real investment in breastfeeding support, safe sleep education, and infant nutrition from birth onward — recognizing that what happens in the weeks after birth matters as much as what happens during it.
The women in those countries are not choosing between natural birth and safety. They are getting both, because the system is designed to support physiology first and escalate only when necessary.
The Breastfeeding Thread — and What It Has to Do With All of This
I want to stay with the milk question a little longer, because I think it belongs in this conversation more than it usually gets to.
I breastfed both of my sons for eighteen months each. And I want to be honest about what that actually looked like with Lucas, because sanitized accounts of breastfeeding do a disservice to women who are trying to make it work and wondering what is wrong with them.
It took seven to nine weeks to get a reliable latch. Seven to nine weeks of cracked, bleeding nipples — I desperately needed the nipple balm I now make, and didn't have it. Of a baby who couldn't latch consistently, of wondering every single feeding whether this was going to work. I did what is called triple feeding: every two hours, around the clock, I pumped, attempted a latch, and fed whatever I had expressed. Each session took an hour and a half or more. Eight times a day. That is twelve hours out of every twenty-four, for more than two months, just to establish feeding. I froze milk in daily bags so I only had to wash pump parts once — the kind of logistical problem-solving that becomes your entire mental landscape in those weeks.
In the hospital, I had asked for a lactation consultant — my friend told me to do this immediately, and I'm grateful she did. There was one consultant for the entire floor. She could give us twenty minutes before discharge. I watched her and the nurse exchange a look that said: we have twenty minutes to fix this. We did not fix it in twenty minutes. We went home without a reliable latch.
We hired a private lactation consultant. Three hundred and fifty dollars, worth every cent, the best money we spent in that first month. She came to our home, watched feeding after feeding, gave us real tools and real reassurance. And still it took weeks.
What broke it open was not technique. It was Lucas. One day — I remember the exact moment — something clicked for him. His eyebrows went up. He finally understood what he was supposed to be doing. He just needed his own time to figure it out, and no amount of better positioning on my part could have moved that timeline.
I had a particular image in my mind that helped me stay determined through those weeks. I had heard about a woman on a plane stuck on a tarmac, with a formula-fed newborn and no water to mix the formula. The baby was screaming. There was nothing she could do. I thought about that image often. I wanted to be able to run anywhere, carry nothing, and have everything my baby needed just by holding him. That freedom — that complete self-sufficiency of the nursing relationship — was worth everything it cost me to get there.
Human milk does not require refrigeration, a supply chain, clean water, or careful handling. It adjusts its composition based on the age of the infant and the pathogens the mother has recently encountered. It is never contaminated between source and baby. The infant drinking directly from the breast is receiving something no formula replicates — not because formula is evil, but because what the breast produces is genuinely, biologically extraordinary.
The second time, with Jaden, was easier from the start. And still — bleeding nipples on the first night. Both children.
The hospital lactation support situation is its own indictment of how we treat the postpartum period. One consultant for an entire floor. Twenty minutes before discharge. The knowledge exists. The staffing doesn't follow it. This, too, is a systems problem, not an individual one.
What I Actually Concluded
Modern medicine has saved enormous numbers of lives — maternal and infant — primarily through sanitation, infection control, nutrition, clean water, and the ability to manage genuine obstetric emergencies. These gains are real, important, and irreversible.
The specific practices that define standard American hospital birth — routine Pitocin augmentation, prophylactic IV lines, continuous electronic fetal monitoring, epidurals as default, cesarean rates double what medical necessity requires — are not primarily responsible for those gains. And in some cases, they contribute to worse outcomes, not better ones.
The countries with the best maternal and infant outcomes today are not the most interventionist. They are the most supportive — of physiological birth, of midwife-led care, of continuous labor support, of breastfeeding, of the postpartum period as a time requiring real investment and rest. They spend less and save more.
The United States has built an extraordinary system for the 10 to 20 percent of births where something goes wrong. It has not built a system that serves the 80 to 90 percent of births where, if left well-supported and minimally disturbed, nothing would go wrong at all.
That is the gap. That is what we could do better. And it does not require technology we don't have — it requires a philosophy we have largely discarded, and an honest willingness to look at the countries that kept it.
Every number in this piece represents a real person. Every maternal death is a family without a mother. Every infant death is a life that didn't get to begin. We owe it to them — and to every woman who will give birth after us — to be accurate about what is actually helping and what is getting in the way.
"The goal is not average care for most. It is best outcomes for most. Those are different things, and the data are clear about which direction to move."
Data sources: OECD Health Statistics 2020/2021; CDC NCHS Vital Statistics; CDC Maternal Mortality Review; ACOG Committee Opinions on Safe Prevention of Primary Cesarean Delivery and Approaches to Limit Intervention During Labor and Birth; Evidence Based Birth (evidencebasedbirth.com); WHO recommendations on intrapartum care for a positive childbirth experience.
Victoria Siegel is a certified community herbalist (California School of Herbal Studies), mechanical engineer, and founder of Rational Body Natural Skincare. She lives in Danville, California with her husband Marcus and their two sons, both born unmedicated in hospital settings. She is currently writing a book on nutrition, birth, and the fourth trimester.
rationalbody.com